Prostate Volume Measurement: TRUS vs MRI Accuracy, Clinical Use, and Calculator Guide
Accurate prostate volume measurement plays a central role in modern urology.
It influences diagnosis, risk assessment, and treatment planning.
Small differences in volume estimation can change clinical decisions.
This article explains TRUS vs MRI for prostate volume estimation in a clear, practical way.
It also explains how a prostate volume calculator works and when to rely on it.
The goal is simple.
Help clinicians, researchers, and informed patients understand accuracy, limitations, and real-world use.
What Is Prostate Volume and Why It Matters
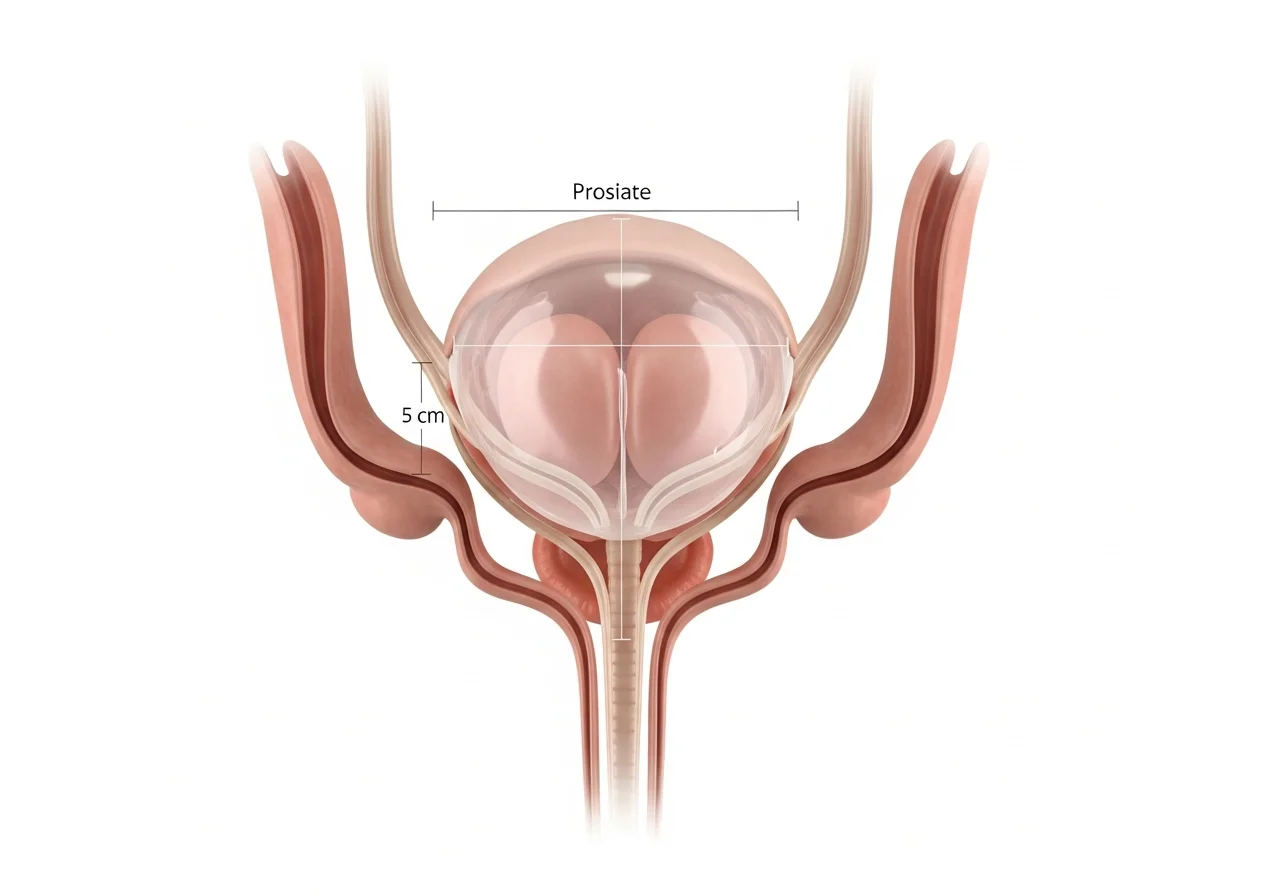
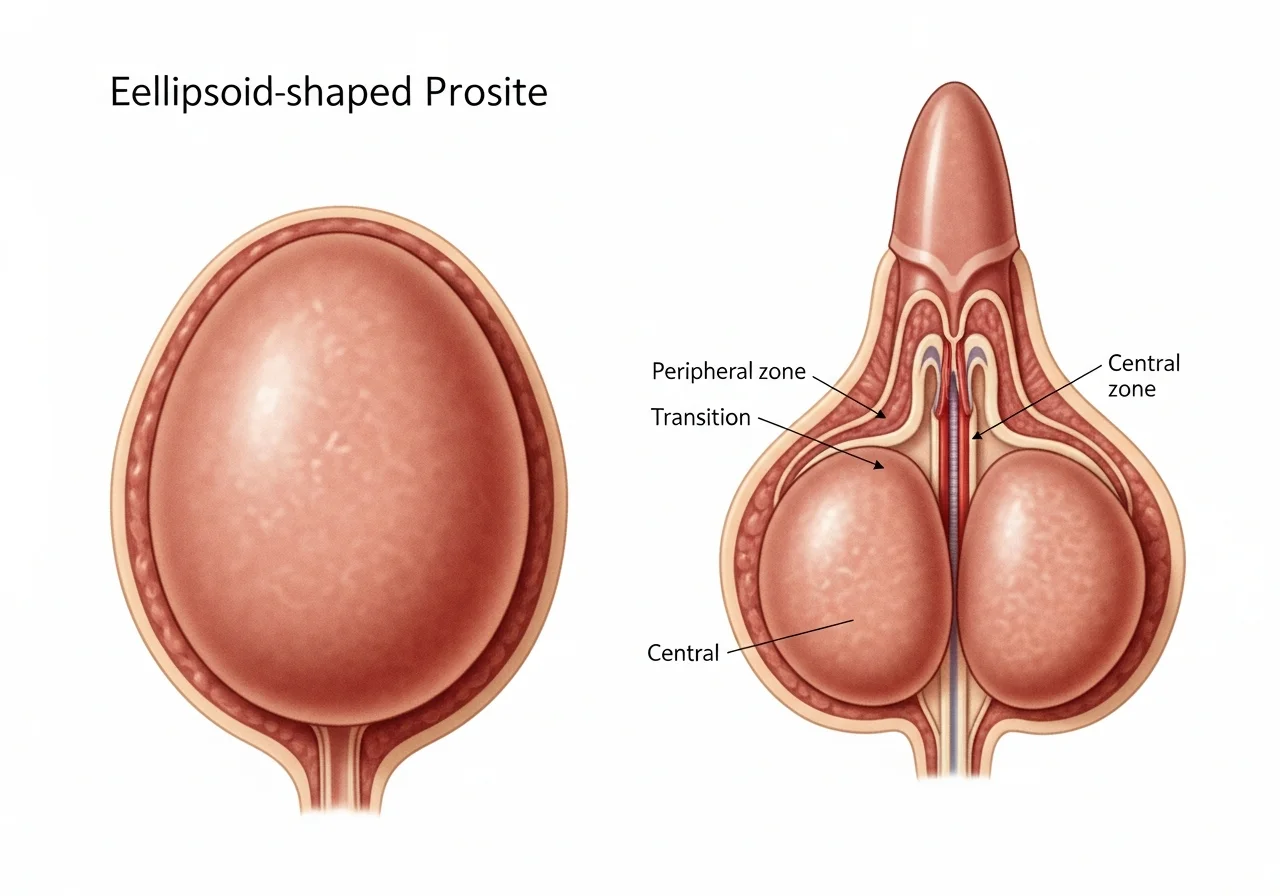
Prostate volume refers to the size of the prostate gland, usually measured in cubic centimeters.
This measurement matters because prostate size affects several clinical decisions.
It directly influences PSA density, which divides PSA by prostate volume.
It helps differentiate benign enlargement from cancer risk.
It guides biopsy decisions and surgical planning.
In benign prostatic hyperplasia, prostate volume helps assess symptom severity.
In prostate cancer, volume affects detection rates and risk stratification.
An inaccurate volume estimate can lead to overdiagnosis or missed disease.
That is why the choice of imaging method matters.
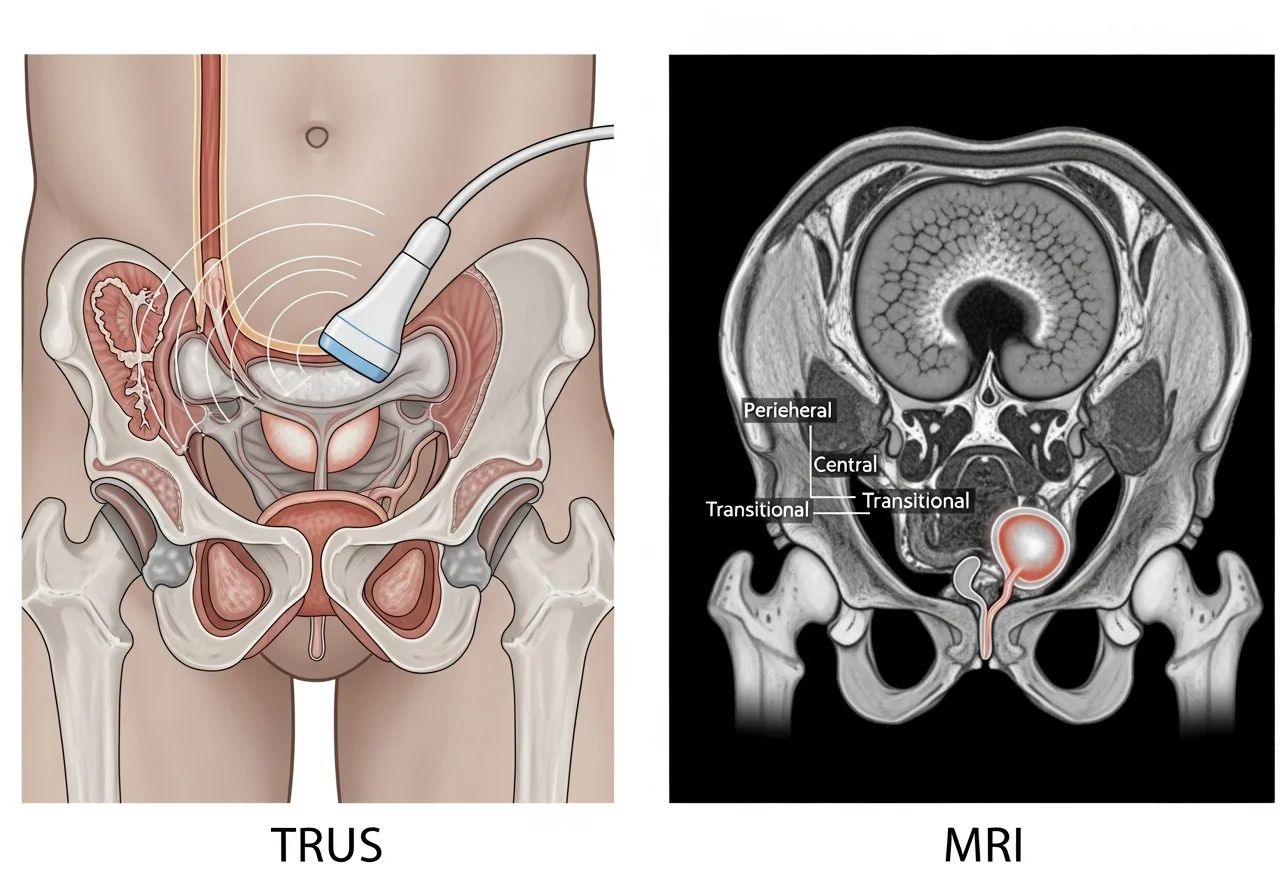
Imaging Methods for Prostate Volume Measurement
Two imaging modalities dominate clinical practice.
Transrectal ultrasound and magnetic resonance imaging.
Each method has strengths and limitations.
Understanding both is essential before comparing accuracy.
Transrectal Ultrasound for Prostate Volume Measurement
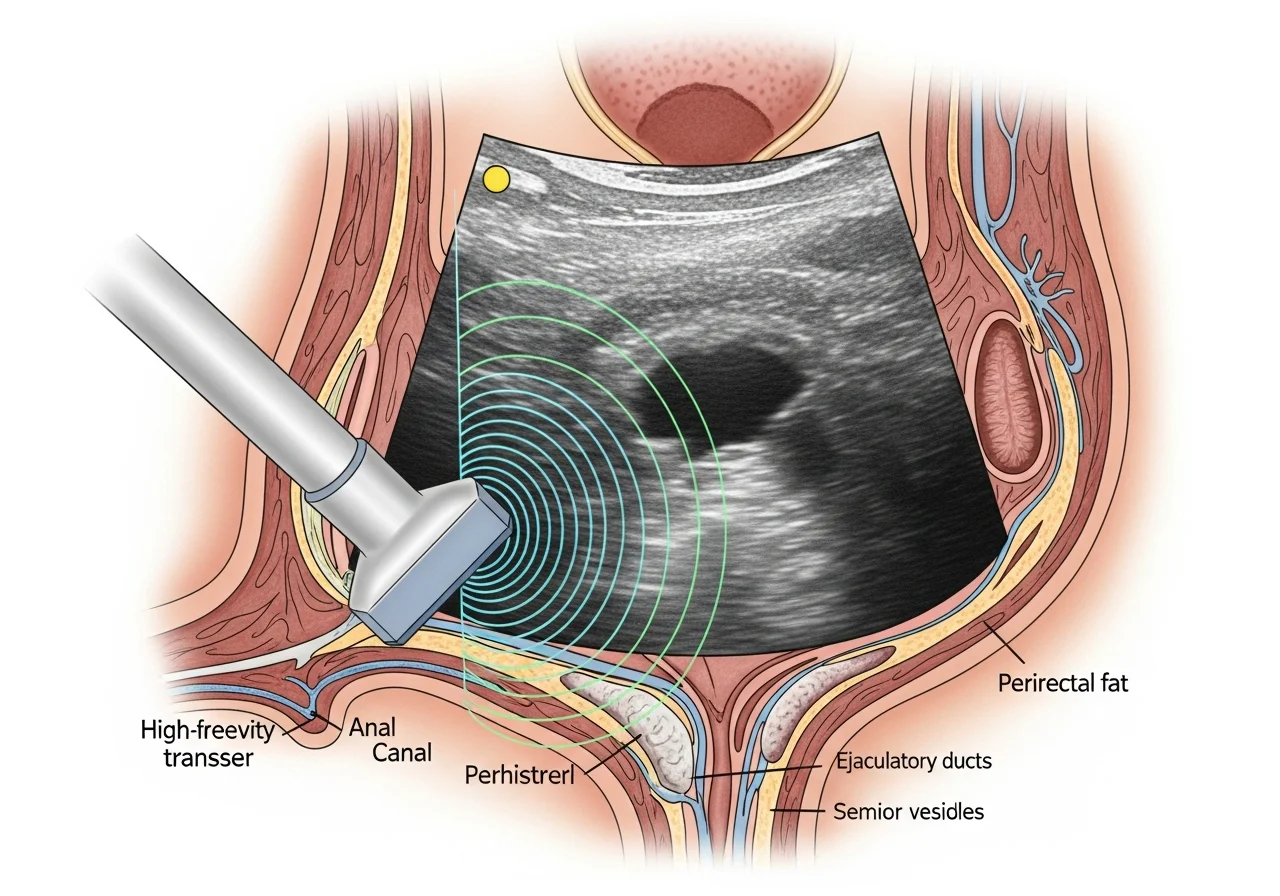
Transrectal ultrasound, commonly called TRUS, uses sound waves to image the prostate.
The probe sits in the rectum.
This position places it close to the gland.
TRUS estimates volume using three dimensions.
Length, width, and height.
These values are applied to the ellipsoid formula.
TRUS prostate volume measurement remains widely used due to accessibility.
Most urology clinics can perform it in the office.
Strengths of TRUS
TRUS is fast.
It is relatively inexpensive.
It integrates easily with prostate biopsy.
It allows real-time imaging during procedures.
For routine assessments, TRUS offers acceptable precision.
This is especially true for small to moderate gland sizes.
Limitations of TRUS
TRUS has known weaknesses.
Visualization of the prostate apex and base can be challenging.
Field of view limits accuracy in larger prostates.
Operator experience influences results.
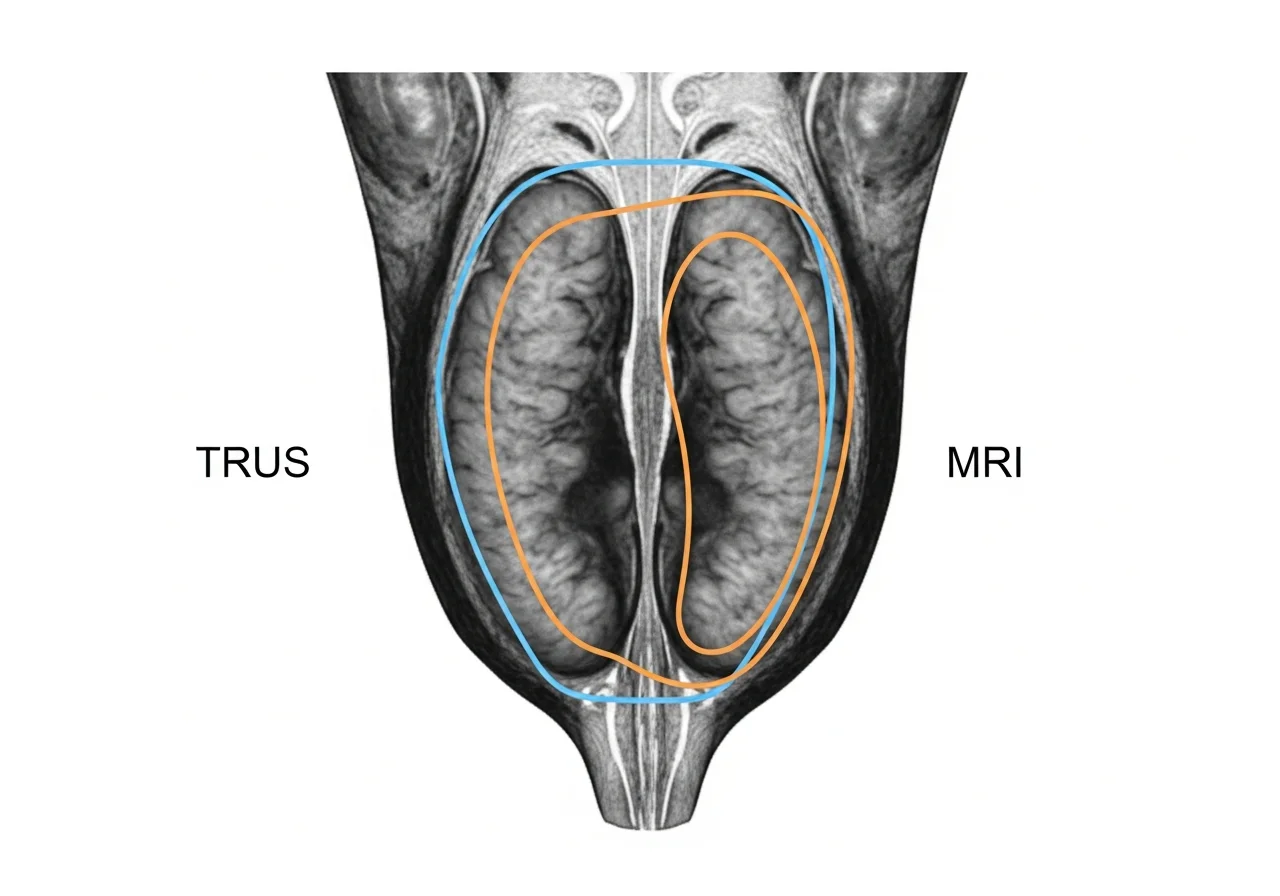
Studies consistently show TRUS underestimates prostate volume, especially in large glands.
This bias affects PSA density calculations.
Magnetic Resonance Imaging for Prostate Volume Measurement
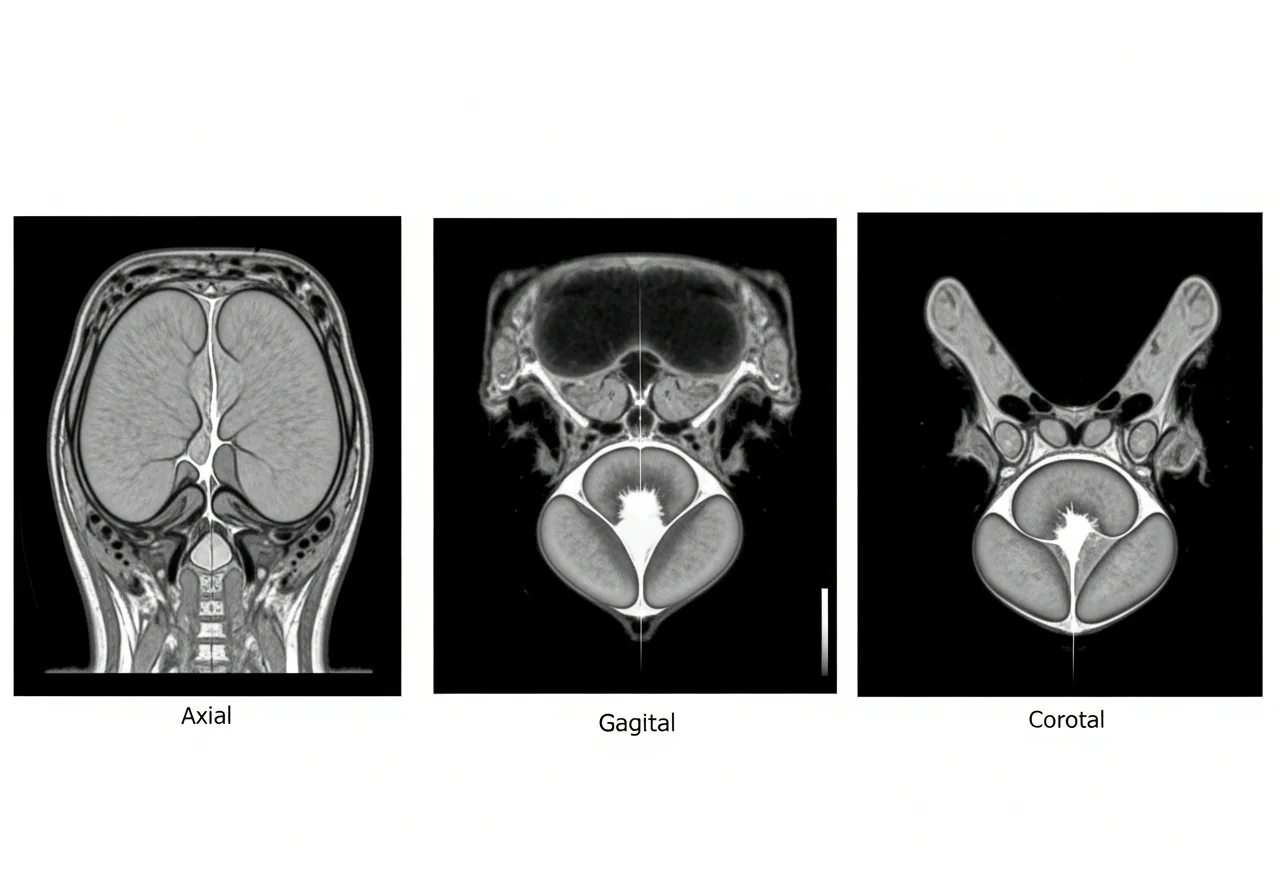
Magnetic resonance imaging, often performed as mpMRI, offers superior soft-tissue contrast.
MRI captures the prostate in multiple planes.
Axial, sagittal, and coronal views provide complete anatomy.
MRI also uses the ellipsoid formula in most clinical workflows.
However, landmarks are easier to define.
Strengths of MRI
MRI visualizes the prostate apex and base clearly.
This improves length measurement.
It reduces interobserver variability.
Different readers produce more consistent results.
MRI shows stronger correlation with surgical specimen weight.
This makes MRI prostate volume more accurate.
Limitations of MRI
MRI costs more than TRUS.
Access may be limited.
Scan time is longer.
Some patients cannot tolerate MRI.
Despite these limits, MRI accuracy offers clinical advantages in selected cases.
TRUS vs MRI: Evidence Based Accuracy Comparison
The debate around TRUS vs MRI focuses on accuracy.
Large multicenter studies now provide clarity.
Correlation With Radical Prostatectomy Specimens
Surgical specimen weight provides a reliable reference.
It represents the true gland size.
Multiple studies compared imaging estimates with prostatectomy specimens.
MRI prostate volume estimation shows higher correlation coefficients.
Values commonly exceed 0.90.
TRUS prostate volume estimation shows lower correlation.
Values range between 0.75 and 0.85.
This difference reflects anatomical visualization.
MRI better captures true gland boundaries.
Underestimation Patterns in Larger Prostates
Prostate size affects measurement accuracy.
In prostates under 50 cc, TRUS performs reasonably well.
Bias remains small.
In prostates above 50 to 80 cc, TRUS underestimation increases sharply.
Some studies report underestimation exceeding 30 percent.
MRI maintains better accuracy across size ranges.
This makes MRI valuable for surgical planning.
Interobserver and Intraobserver Reliability
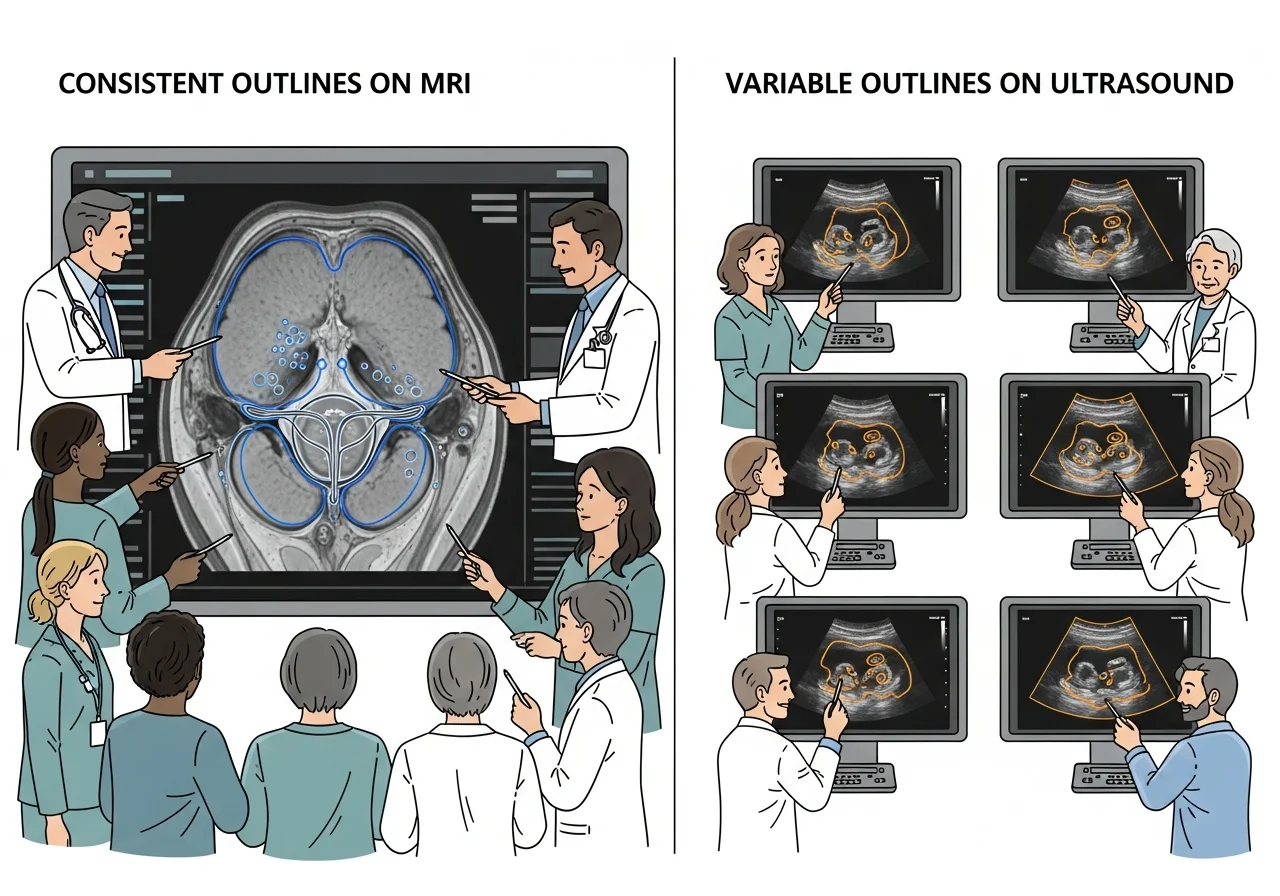
Consistency matters in clinical practice.
MRI shows higher interobserver agreement.
Different readers reach similar volume estimates.
TRUS results vary more between operators.
Probe positioning and landmark selection matter.
For follow-up and research, reproducibility matters.
MRI performs better in this area.
Prostate Volume Calculation Methods
Imaging provides dimensions.
Formulas convert dimensions into volume.
Understanding formulas helps interpret calculator results.
Ellipsoid Formula for Prostate Volume
The ellipsoid formula is widely used.
Volume equals length times width times height times 0.52.
This method assumes the prostate resembles an ellipsoid.
That assumption often fails.
Many prostates show asymmetric enlargement.
Transition zone growth distorts shape.
Despite limitations, the ellipsoid formula remains standard.
Both TRUS and MRI rely on it.
Bullet Formula for Prostate Volume
The bullet formula adjusts the shape assumption.
It multiplies dimensions by 0.65 instead of 0.52.
This correction improves accuracy in larger glands.
Especially those with adenomatous enlargement.
Studies suggest the bullet formula reduces TRUS bias.
It aligns estimates closer to MRI values.
Impact on PSA Density and Cancer Detection
Prostate specific antigen density depends on volume accuracy.
PSAD equals PSA divided by prostate volume.
Small errors in volume lead to large PSAD shifts.
TRUS Based PSAD vs MRI Based PSAD
When TRUS underestimates volume, PSAD rises artificially.
This may trigger unnecessary biopsy.
MRI based PSAD often lowers density values.
Some patients cross below biopsy thresholds.
Studies show reclassification rates near 20 percent.
This affects clinical decisions.
When PSAD Loses Predictive Value
In very large prostates, PSAD loses reliability.
Volume dominates the equation.
Both TRUS and MRI PSAD perform poorly above certain sizes.
This limits usefulness in advanced BPH.
Understanding these limits prevents overinterpretation.
Clinical Decision Guidance
Imaging choice should match clinical context.
No single modality fits all scenarios.
When TRUS Is Sufficient
TRUS works well for initial evaluation.
It suits routine BPH assessment.
It supports biopsy guidance.
It offers cost efficiency.
For small to moderate glands, TRUS accuracy is acceptable.
Clinical impact remains limited.
When MRI Should Be Preferred
MRI helps in borderline PSAD cases.
It refines biopsy decisions.
MRI improves pre surgical planning.
This includes HoLEP and robotic prostatectomy.
When TRUS and clinical findings conflict, MRI clarifies anatomy.
Prostate Volume Calculator Explained
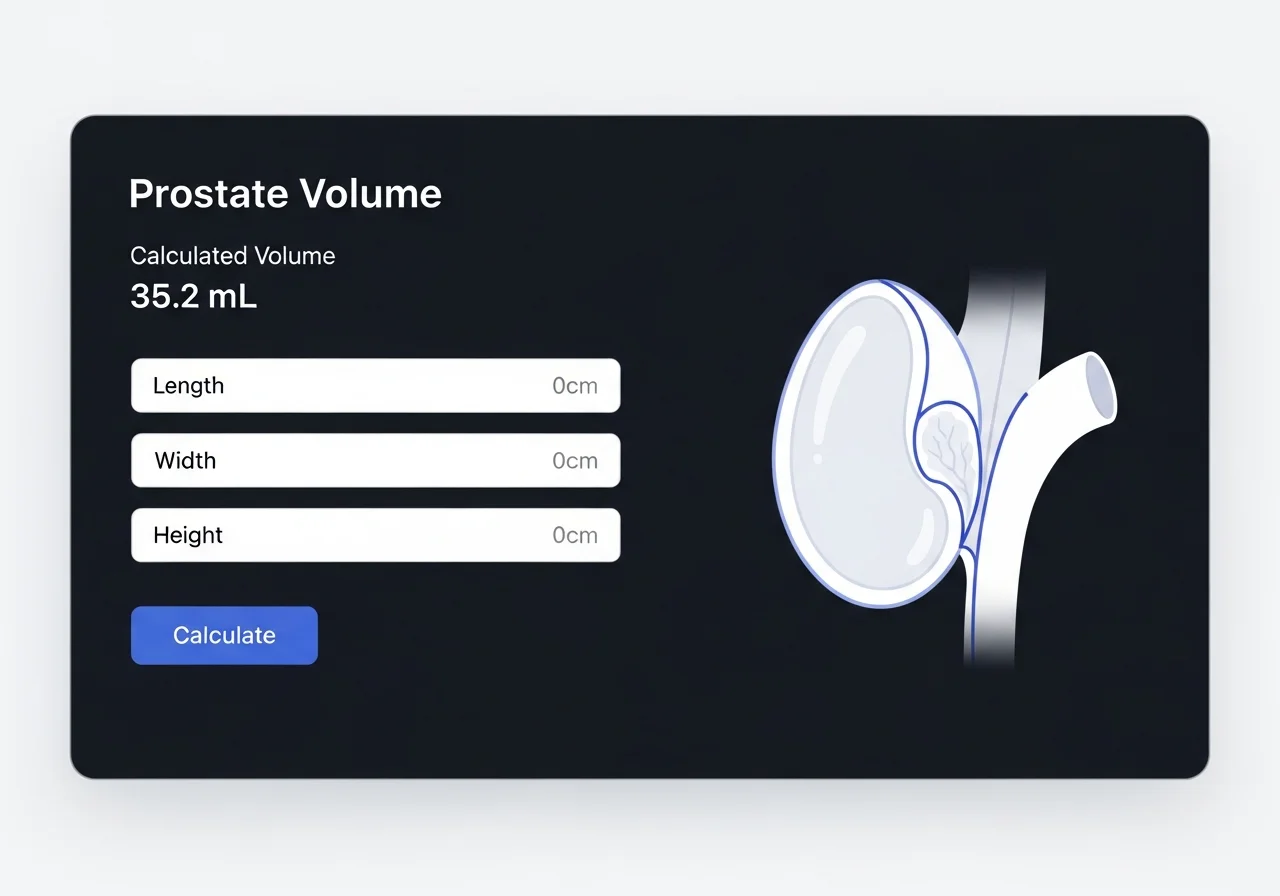
A prostate volume calculator converts measurements into volume.
It accepts dimensions from TRUS or MRI.
Some calculators offer both ellipsoid and bullet options.
How the Prostate Volume Calculator Works
Users enter length, width, and height.
The calculator applies the selected formula.
It outputs prostate volume in cubic centimeters.
Some calculators also compute PSA density.
This helps clinical interpretation.
Interpreting Calculator Results Safely
Calculator accuracy depends on input quality.
Poor measurements yield poor results.
Users should know the imaging source.
TRUS and MRI inputs differ.
Formula choice matters in large prostates.
Bullet formula may reduce bias.
Always interpret results in clinical context.
Avoid rigid thresholds.
Common Errors in Prostate Volume Measurement
Errors arise from anatomy and technique.
Apex misidentification shortens length.
Base misalignment inflates height.
Including bladder tissue skews results.
Ignoring intravesical protrusion causes bias.
Assuming all prostates are ellipsoids introduces error.
Shape variability matters.
Understanding these pitfalls improves interpretation.
Accuracy and Reliability Considerations
No imaging method is perfect.
MRI offers higher accuracy but lower availability.
TRUS offers speed but lower precision.
Reliability improves with experience.
Standardized measurement protocols help.
Advanced segmentation tools may improve future accuracy.
Clinical adoption remains limited.
Real World Use Cases
Consider a patient with PSA of 6.0.
TRUS estimates volume at 40 cc.
PSAD equals 0.15.
Biopsy appears indicated.
MRI estimates volume at 55 cc.
PSAD drops to 0.11.
Clinical decision changes.
Biopsy may be deferred.
This illustrates why MRI vs TRUS prostate volume matters.
Benefits and Limitations Summary
TRUS benefits include accessibility and integration.
Limitations include underestimation bias.
MRI benefits include anatomical precision and reproducibility.
Limitations include cost and access.
Using both wisely improves care.
Frequently Asked Questions
Is MRI more accurate than TRUS for prostate volume
Yes.
Most studies show MRI correlates better with specimen weight.
Does TRUS underestimate prostate volume
Yes.
Underestimation increases in larger prostates.
Which formula should be used for PSA density
Ellipsoid remains standard.
Bullet formula may help in large glands.
When should MRI replace TRUS
Use MRI for borderline PSAD or surgical planning.
Key Takeaways
Accurate prostate volume measurement matters.
It influences diagnosis and treatment.
TRUS vs MRI is not a competition.
Each serves a role.
MRI offers higher accuracy.
TRUS remains practical.
Understanding formulas and limitations improves decisions.
Tools help when used correctly.
References and Evidence Base
This article draws from peer reviewed urology research.
Multicenter studies support the conclusions.
Guidance aligns with established urologic practice standards.
Readers should consult clinical guidelines for decision making.
Final Note
This guide aims to explain prostate volume estimation clearly.
It supports clinicians and informed users alike.
Accurate measurement starts with understanding.
Understanding leads to better care.